

On Thursday July 17th yet another high-profile cyclist was thrown out of the Tour de France when Riccardo Ricco was taken into custody by the French gendarmes after he tested positive for a synthetic variant of EPO. This post is in no way intended to express sympathy for Ricco or to argue that what he apparently did was justified. As the rules currently stand EPO is a banned substance. Riders who use it are cheating and they should be kicked out of the race. Unless the drug test was a false positive, Ricco got what he deserved. Throw the bums out.
The issue I want to consider here is not whether Ricco should have been punished, but whether blood doping and the use of EPO should be prohibited as forms of performance enhancement. They are currently banned and there are good arguments for continuing to do so. However, I think there is an alternative way to look at doping and EPO that should be considered.

The use of performance enhancing drugs in competitive sports is an enormous problem. Many professional sports are addressing the problem by identifying banned substances, instituting testing procedures for those substances and legislating penalties to be applied to athletes who are found to have used the banned drugs. From professional leagues that are more interested in maintaining the image of being anti-drug than in actually dealing with the problem, to drug tests that are often not conclusive, to athletes that lie about their drug use or insist they didn’t know they were taking a banned substance the problem of performance enhancing drugs in sport seems almost impossible to solve.
And this is only the tip of a much larger iceberg. I think consideration of this issue opens up a world of deeper questions about what constitues performance enhancement, whether some practices that are currently considered as illegal forms of enhancement might be acceptable or even desirable at some levels of sporting competition, and what functions we want different levels of sporting competition to fulfill in our culture. Consider the following.
One of the desired ideals for sporting competition is that the competitors should begin from a level playing field, that none of the athletes be given an unfair advantage over the others. The competition begins on a level playing field and the athlete who has trained harder, who understands the game better, who is more skilled, who is better able to maintain focus during the heat of the battle wins in the end. At least that’s the way it should be. A fundamental objection to the use of performance enhancing drugs is that they upset this level playing field by giving the drug user an advantage that is not due to his training, knowledge or skill. Is this always true? It depends on how you look at it.
The amount of oxygen carried by the blood is an essential determinant of performance in sports. Oxygen is used to both carry energy to the muscles so that they can perform the work the sport requires and to carry waste products away from the muscles. Oxygen carrying capacity is especially important in long term endurance events such as road racing in cycling where athletes must sustain very high levels of performance for hours without a break. Many world-class athletes in high endurance sports have used artifical means to increase their oxygen carrying capacity in order to gain what can be a substantial competitive advantage.

Red blood cells
Oxygen is carried in the blood by red blood cells (RBCs) and an increase in the density of RBCs in the blood can greatly improve performance in endurance sports. The two methods most commonly used to do this are blood doping and the the injection of EPO (erythropoietin). Blood doping involves extracting blood from a donor, concentrating the blood so that it has a high proportion of RBCs, freezing the concentrate and then thawing it and injecting it into the athlete before the competion or during the competition in the case of multi-day events such as the Tour de France. The donor can be either the athlete himself (autologous blood doping) or someone else with a compatible blood type (homologous blood doping). EPO is a hormone that is naturally produced by the kidneys and that stimulates the production of RBCs in the bone marrow. EPO can also be made in the laboratory and this type of pharmaceutical EPO can be injected under the skin to increase the body’s RBC production. Ricco was charged with taking a variant of pharmaceutical EPO called CERA.
The use of EPO or blood doping can be difficult to detect. Subcutaneously injected EPO typically cannot be detected 3 to 4 days after injection yet it has its maximum effect stimulating high levels of RBC production approximately 3 weeks later. For that reason, banning an athlete for EPO use usually depends on catching him with EPO paraphanalia in his possession. In Ricco’s case, the manufacturer, F. Hoffman-La Roche, worked with WADA (World Anti-Doping Agency) to develop a test for the drug. Homologous blood doping (using someone else’s blood) can be detected by DNA differences between the donor and the athlete’s RBCs. Autologous blood doping (using your own blood) is extremely difficult to detect and no tests are currently available that are considered reliable enough to use in competitive sports.
In addition to relying on blood tests that are specific for EPO use or doping many professional sports use hematocrit as an indicator of illegal performance enhancement. Hematocrit measures the proportion of the blood volume that is composed of RBCs. Hematocrits above a certain level are taken to be abnormal and are officially used as indicators of doping or EPO use. The UCI (Union Cycliste Internationale), the organizing body of professional cycling, has set 50% as the upper allowable hematocrit level. If a rider tests with a hematocrit above 50, he is banned from competition.
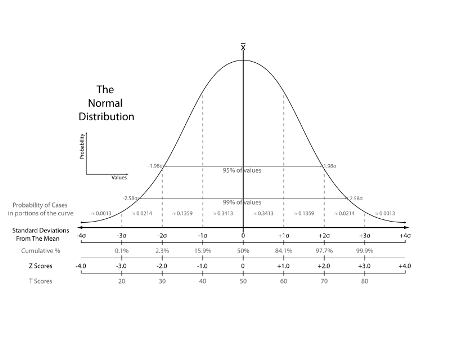
It is often cited that the “normal” hematocrit range in adult males is between 41 and 50. This is the two standard deviation range which encompasses approximately two thirds of the general population. The upper level of the three standard deviation range for hematocrit is 54. Approximately one third of the general population falls outside the two standard deviation range that is cited as “normal”. More to the point, approximately one sixth of the general population (about 16.6%) will have naturally occurring hematocrit levels above 50. We can also expect that those individuals with higher than normal hematocrit levels will be disproportionately represented in the population of endurance athletes because the increased oxygen carrying capacity of their blood gives them a natural advantage in endurance sports. The UCI recognizes this problem by allowing exceptions to the 50 hematocrit rule for cyclists who have a long and consistent history of hematocrit measures above 50 as indicative of a naturally occuring high hematocrit level.
All professional endurance sports ban both EPO and blood doping as illegal forms of performance enhancement. Should they do this? If we consider them as a means of gaining an unfair advantage over the opponent, which is the way they are currently used, the answer is clearly “yes”. However, I think another perspective is possible.
Everyone has a naturally occuring hematocrit level that is genetically determined. This natural hematocrit is not subject to training, it is what it is. Natural factors such as training at high altitude or anemia, and artificial factors such as the use of EPO and blood doping can temporarily increase or decrease hematocrit but they do not affect the base hematocrit that each of us is born with. This means that independently of any steps the competitor may take to increase hematocrit, some endurance athletes have a competitive advantage because of their genetics. In other words, with all other things such as training regimen, skill level, knowledge of the sport, strength of will and competitive focus held equal, the endurance athlete with a naturally high hematocrit will have an advantage over the athlete who was born with a low hematocrit.
With regard to hematocrit, a critically important factor in endurance sports, the playing field is not level. The low hematocrit athlete starts at a disadvantage that has nothing whatsoever to do with anything that is relevant to the sport. It’s not about training regimen or intensity, it’s not about knowledge of the sport, the competition or the opponent, it’s not about trained skills and it’s not about heart, will or desire. It’s about which sperm happened to fertilize which egg when the athlete was conceived.
Suppose we shift the common perspective on the use of EPO and blood doping. Rather than think of them as a means to unbalance the competition by giving an athlete an unfair advantage, suppose we think of them as medical technologies we can use to level the playing field so that some athletes don’t begin the competition at a marked disadvantage because of their genetic inheritance? Viewed from this different perspective, EPO and blood doping could be used to bring all of the athletes up to the same hematocrit level so that the competition could be decided on the basis of factors the athlete can control such as training, knowledge and desire.
Under the current system EPO and blood doping are used surreptitiously by some athletes to give them an unfair advantage over their opponents. These techniques unbalance the playing field. However, if we make EPO and blood doping available to any athlete who wants to use them, these technologies can eliminate a naturally occurring advantage that benefits some athletes but not others. The technologies level the playing field.
How might EPO or blood doping be used in this way? Set a hematocrit level as a cut off point such as the level of 50 currently used by the UCI. Competitors may use any means they wish such as training at altitude or using EPO to bring their hematocrit up to this level. The athelete is tested before every competition, or in multi-day events such as the Tour de France before every stage, and they must have a hematocrit level below the cut off. Under this system hematocrit level would function like weight levels in wrestling or boxing. If you don’t make level, you can’t compete in the event. You’re not labled as a cheater, fined and banned from the sport. You simply cannot compete in the current event because your hematocrit level gives you an unfair advantage.
This approach to the problem has several advantages. First, by reorienting our thinking away from the view that these medical technologies are a means of introducing unfair advantage to the view that they are a means of eliminating unfair advantage we reorient the relationship between the athlete and his sport. The athlete is no longer a cheater who is afraid of discovery and the organizing body of the sport is no longer treating its athletes like criminals to be caught. Second, medical technologies that currently are used in secret and not in the best and safest of ways would be used in the open and in much safer conditions. Third, as athletes strain to get as close to the cut off point as possible without going over and being eliminated from competition, our knowledge of how to use technologies like EPO and blood doping would increase and the conditions under which these technologies can be safely used would become better understood. Fourth, and perhaps most important of all, a playing field unbalanced by genetic factors is leveled so that competitions are less likely to be determined by the DNA of the athlete’s parents and more likely to depend on what the athlete has done to prepare for the event.
The underlying issue here is how professional sports in general and cycling in particular should respond to advances in our scientific understanding of the anatomical and physiological factors that affect athletic performance and the medical technologies that are developed from this understanding. New technologies in the fields of drug treatments, prosthetics, and genetic engineering have the potential to substantially alter human capabilities and performance levels. How should sport respond to this advancing knowledge? One possibility is that medical technologies could be evaluated individually to determine whether they can be used to enhance fair competition if made available to all of the competitors as opposed to unbalancing competition when they are only used by those who are willing to cheat.
Is this the right way to think about EPO and blood doping? I don’t know but it’s worth considering.


